Is Partial Knee Replacement What You Need?
By Mr. Sam Rajaratnam FRCS (Tr. & Ortho)
Knee replacement is needed when the joint has become so worn, damaged or diseased that, having tried and failed to relieve the pain with non-invasive treatments, the patient finds it too painful carry out everyday activities and the joint is unstable. The most common reason for knee replacement is osteoarthritis, (96% of patients according to the National Joint Registry (NJR) 15th Annual Report 2018 ). However, knee replacement can also be considered for any condition such as trauma, rheumatoid arthritis or any other inflammatory disease of the knee joint, which prevents the patient from using the joint without pain.
The knee is composed of three compartments. Partial knee replacement, also called unicompartmental knee replacement (UKR) or unicompartmental knee arthroplasty (UKA), is the term used when the bone and/or articular cartilage in just one of these compartments is resurfaced. The alternative to a partial knee replacement is a complete replacement of the knee, called total knee arthroplasty (TKA). TKA is by far the most common knee replacement procedure carried out in the UK. The NJR 15th Annual Report 2018 states that of 1.08 million primary knee replacement procedures recorded approximately 90% are for TKA and just 10% for partial knee replacement.
There is also a much less common procedure for early-stage osteoarthritis called osteotomy but it is suitable only if one compartment of the knee is affected. Here a wedge of bone is removed from the femur or tibia in order to redistribute the pressure in the knee joint. The number of patients recorded in the United Kingdom Knee Osteotomy Registry between 1st December 2014 and 1st December 2017 was 1,652. As a comparison in the three years 1st January 2015 to 31st December 2018 there were 272,133 primary total knee replacements carried out and 28,573 partial knee replacements.
THE REASON FOR PARTIAL KNEE REPLACEMENT
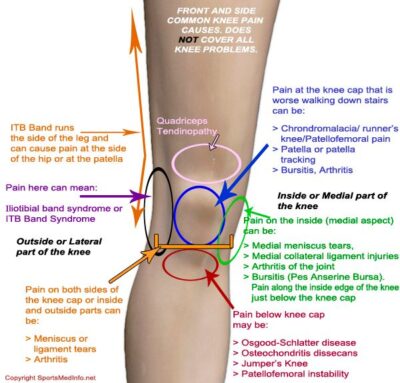
The three compartments in the knee are named after three bones which form each compartment and its location. There is, therefore, the patellofemoral compartment, which lies between the femur and the patella, the medial femorotibial compartment, on the inside of the knee between the femur and tibia, and the lateral femorotibial compartment on the outside of the knee.
If the articular cartilage in one of these compartments becomes worn and breaks down the body tries to repair itself creating changes within the joint. These changes can include extra fluid being produced by the lining of the joint capsule causing the joint to swell, stretching of the tissue around the joint causing instability, and the development of bony spurs (osteophytes) causing pain and a reduction in joint flexibility. If this occurs it may be decided that a UKA or TKA is appropriate.
ADVANTAGES AND DISADVANTAGES OF PARTIAL KNEE REPLACEMENT
The advantages of a unicompartmental knee replacement may seem attractive as they can include reduced surgical invasive procedure leading to less blood loss, less soft tissue and bone dissection, quicker recovery time and a reputed more natural feeling in the knee. However, there are disadvantages as well. The procedure is not as predictable for pain relief as TKA and there may be complications later such as arthritis progressing in other compartments. If arthritis does progress a subsequent TKA will be needed, and indeed figures suggest a higher risk of further surgery being needed following a partial knee replacement. The NJR figures show that the risk of a revision (i.e. a second, corrective, operation) is significantly higher for partial medial or partial lateral replacements than for TKA. Patellofemoral revision figures are even higher. The NJR report states that there should be an element of caution in thinking that a partial replacement can be used as an interim procedure or as a lesser intervention than a TKA. This is because the risk of re-revision after a revision procedure is higher for partial replacements than the risk of a revision for a primary TKA.
RISKS OF PARTIAL KNEE REPLACEMENT AND TKA
All surgery comes with risk, and knee surgery is no different. The main risk of a partial knee replacement is that the patient may have ongoing pain or wear from the rest of the knee joint and thus may need further surgery to address the issue. This subsequent revision may not be straightforward and is often more complicated than a direct TKA.
Mr Rajaratnam performs both partial and total knee replacement surgery and is one of the leading joint replacement experts in the country with amongst the lowest revision rates for his surgery on the National Joint Registry. He is ideally placed to carefully assess each knee and recommend the option which is likely to be the most successful for each individual patient.
PARTIAL KNEE REPLACEMENT SUCCESS RATES
If we are considering partial knee replacement success in terms of longevity, it does not last as long as TKA. A study, carried out by the Musculoskeletal Research Unit at Bristol University, has recently been published which includes case studies from over 25 years on 500,000 patients. It showed that for partial knee replacements 77% lasted 15 years, 72% lasted 20 years and 70% lasted 25 years. In the study this compares unfavourably with TKAs, which were found in 93% of the cases to last 15 years, 90% lasted 20 years and 82% lasted 25 years.
In terms of the need for revision, the risk of revision for a partial knee replacement is at least two times higher than for a TKA.
WHO IS PARTIAL KNEE REPLACEMENT RIGHT FOR?
There is no definitive answer to this question because every case is unique in terms of the clinical problems presented and the personal circumstances of the patient. It has been advocated that partial knee replacement is most suitable for patients at both extreme ends of the age range. Suggestions have been made that the procedure would be best for younger patients because their age means that their recovery will be quicker and involve much less pain. Conversely, it is also said that it is best for older patients because they no longer need to engage in strenuous activity. However, in the case of younger patients, if there is a need for revision surgery and TKA, the previous surgery can make this revision more difficult. In older patients, if degeneration of the joint is already present, there is the possibility of further progression, and again any partial replacement may complicate subsequent TKA. UKA may be an option for older patients who are not going to engage in heavy manual work or punishing sporting activities, but this has to be balanced against the possibility of a revision sometime in the future. The only possible answer is that partial knee replacement can be a solution for the right patient at the right time. However, the figures show that there are about ten times more TKAs than UKAs which indicates that a TKA, in the right circumstances, is often more likely to provide the patient with a trouble-free outcome without the need for further intervention.
If you are concerned about pain or problems in your knee, Mr Rajaratnam welcomes patients who require a careful and considered second opinion.