Anterior Knee Pain
By Mr. Sam Rajaratnam FRCS (Tr. & Ortho)
Anterior knee pain or patellofemoral pain syndrome (PFPS) is often the most common cause of knee pain encountered at presentation which does not have a specific traumatic cause.
Brief Structure of the Knee Joint
The ridge at the back of the patella (kneecap) fits into the trochlear groove in the femur and floats between the femoral condyles (raised ridges) at the distal end of the femur. The patella is held in position by the patella tendon and other soft tissue structures.
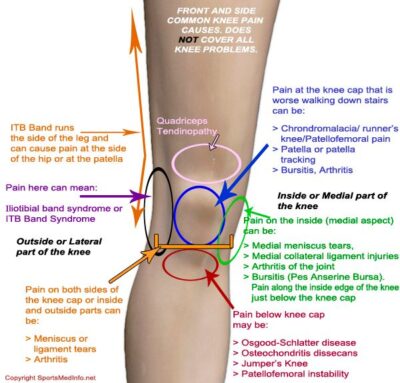
Causes of Anterior Knee Pain
The causes of anterior knee pain can be varied. From biomechanical causes such as altered movements of the hip, knee, ankle or foot to weakened muscles of the thigh, bone abnormalities, arthritis or other inflammatory conditions.
Displacement and Pressure on the Patella
Biomechanics
One of the most common causes of anterior knee pain is poor biomechanics and poor foot posture. When walking, your arches, which occur on the median side of the foot, are very important in weight bearing and help to disperse the impact forces throughout the body. As the foot lands normally on the outside of the heel, movement continues through the mid part of the step at which point the body’s weight travels directly down through the leg causing the toes to splay and absorb the shock. At this point the tibia and femur are rotating about the knee joint. The weight then rolls across the foot to the median side, where the big toe is activated to propel the body forward. The arch allows the foot to splay and absorb the impact forces, and the femur and tibia must be rotating correctly or the patella will be pulled out of line. Correct foot biomechanics have a considerable effect on the knee joint because forces are moved upward into the knee and beyond. Increased weight bearing increases the forces behind the kneecap. Therefore poor foot posture has a direct influence on the forces on the kneecap, and may initiate problems in that area. Changing foot dynamics may well reduce this sort of pain.
Skeletal Problems
Associated with biomechanical problems are skeletal malalignment issues with the tibia and fibula. These can be an (outward) valgus deformity of the distal part of the leg below the knee joint or an (inward) varus deformity of the distal part of the leg. Any deformity alters the mechanics of weight distribution through the hip and leg, and alters the setting of the patella in the trochlea groove. There may well be underlying conditions for these skeletal problems which can be treated e.g. Vitamin D for rickets, but some problems can sometimes be alleviated by orthotics.
Bipartite patella is a congenital condition which occurs when the two parts of the patella remain separate and do not fuse as the child grows. It is quite rare and tends to affect males more than females.
Muscle and Tendon Problems
Unequal muscle and tendon tension either to the side or to front and back of the knee joint can cause pressure on the patella.
Quadriceps and hamstring muscle tightness can affect what happens to the kneecap. Tightening of the hamstring, at the back of the leg, increases the forces on the front of the kneecap causing pressure in this area.
Similarly quadriceps muscle tightening at the front of the leg leads to increased pressure on the quadriceps tendon and patellar tendon. This tightness leads to compression forces on the kneecap. Both these factors result in pain in the front of the knee.
Overstretching of the patellar tendon can also cause pain (patellar tendonitis or tendinopathy). This usually occurs particularly in teenage males who are active in sports, and is due to repetitive loading of the patellar tendon.
Another cause of patella misalignment is an unequal pull between the vastus lateralis and the iliotibial band on the outside of the thigh, and the vastus medialis obliquus on the inside. This causes the patella to track outside the trochlear groove.
All these muscle and tendon problems can also lead to pain due to increased wear on the trochlear groove because the patella is not tracking smoothly. After a period of time the cartilage in the trochlear groove and that on the underside of the patella may wear away causing the bones to come in contact and resulting in patellofemoral arthritis.
In addition, any roughness at the back of the patella or in the trochlear groove causes a grinding which can be heard, and is called crepitus. This can lead to bone erosion and can happen at any age, but is more common in older people. An occasional cracking noise in the knee is normal, but if it happens regularly and is painful it may indicate osteoarthritis, rheumatoid arthritis or patella dysfunction.
Inflammatory Causes
There are a number of conditions which cause inflammation to the tendons or underside of the patella or bursae.
Patella Chondromalacia
Prolonged sitting can can cause pressure on the femoral joint so that you feel you have to get up and move your knee. Inflammation at the back of the patella causes pressure which you feel you must relieve by movement. Here the cartilage on the underside of the patella is softened due to pressure or possibly hormonal changes. It produces an aching pain sometimes accompanied by swelling. The condition is sometimes improved with rest and pain medication. It is more common in younger females and when more weight is put on the knee after a growth spurt.
It can be associated with excess lateral pressure where the patella sits outside its usual path and presents as lateral tightness so the the patella does not move easily in a lateral direction when manipulated.
Sometimes an unstable flap of cartilage may cause pain here which can be cured with simple keyhole surgery and a chondroplasty.
Osgood-Schlatter Disease
This is due to inflammation of the patella ligament at the tibial tuberosity. It occurs most commonly in children and adolescents who are active in sports. It usually occurs during growth spurts when bones, tendons and muscles are changing. The patella tendon pulls on the tibial tubercle, and repetitive traction leads to inflammation of the growth plate under the tibial tubercle. It presents as the knee being tender and swollen at the tibial tubercle and the muscles being tight.
Sinding-Larsen-Johansson Syndrome
Sinding-Larsen-Johansson syndrome is similar to Osgood-Schlatter disease in that it is an inflammation of a growth plate, but this time the plate under the attachment of the patella tendon to the kneecap at the inferior pole of the patella (bottom of the kneecap) rather than at the tibial tuberosity, so it occurs at the bottom of the patella rather than at the top of the tibia as in Osgood-Schlatter disease. Similarly to Osgood-Schlatter disease it tends to afflict active teenagers during growth spurts.
Bursitis
The bursae are thin fluid-filled sacs located at points of friction between bone and the surrounding soft tissue. Bursitis is caused by inflammation of a bursa, and this is most common in the bursae at the front of the knee. Once inflamed it can cause a reasonably large swelling on the knee. It is often caused by repeated kneeling, although a trauma or a medical condition can also cause bursitis.
Genetic Cause
Hypermobility Syndrome
Hypermobility syndrome is the ability of joints to move beyond the normal range. There is a tendency for hypermobile joints to be passed on by specific genes from one generation to another. A hypermobile knee joint may present as pain in the knee. There is added risk because hypermobile joints tend to be more prone to injury, and can eventually lead to degenerative cartilage and arthritis.
Common Symptoms
- Pain beneath and around the kneecap especially when walking up and down stairs, kneeling or squatting.
- Clicking or grating of the knee.
- Knee giving way.
- Pain after sitting in the same position for a long time.
- Swelling.
- A tightness in the calves and thighs.
Anterior Knee Pain Treatments
- Activity modification, anti inflammatories, analgesics.
- Orthotics, such as shoe insoles or inserts to cushion shock, and shoes which support the foot and modify rotational forces during walking.
- Physiotherapy-particularly medial quadriceps strengthening – and particularly the vastus medialis obliquus muscle of the inner thigh to keep the patella tracking towards the inside of the knee.
- Injection treatments include corticosteroid to reduce inflammation and for quick pain relief, the effects may last a few months. Hyaluronic acid is a natural substance found in the synovial fluid. Given as a course of injections the relieving effects can last for a few months.
- Surgical Solutions – keyhole surgery and a chondroplasty can commonly be effective for cartilage problems. Arthroscopy is an exploration to see if there is a correctable cause of the problem. Lateral release is a procedure to re-align the kneecap. Patella realignment surgery takes various forms, but major interventions are very rare and only usually occur if the patella is tilting abnormally or in the case of a really bad alignment valgus (knock knee) deformity. In severe cases of osteoarthritis various forms of replacement surgery can be appropriate.